Treatment Options – Surgical
Surgery involving the spine can occur anywhere along a persons vertebral column. This includes their cervical (neck), thoracic (upper back) or lumbar (lower back) spine area. While no surgery is common, our straight forward section discussion types of spinal surgery that is routinely done by Dr. Aslie.
Our complex section outlines procedures which include fusions.
The minimally invasive section describes innovative techniques through smaller incisions.
Anterior Lumbar Interbody Fusion (ALIF)
What is it?
Anterior Lumbar Interbody Fusion (ALIF) is an operation that involves approaching the spine through an incision in the abdomen. A portion of the affected disc space is removed from the spine and replaced with an implant. Titanium or stainless steel screws and rods may be inserted into the back of the spine to supplement the stability of the entire construct.
Why is it done?
Patients who are suffering from back and/or leg pain are potential candidates for the ALIF procedure. This pain is generally caused by natural degeneration of the disc space.
The Operation
The ALIF operation is performed with the patient lying on his or her back.
Incision
The surgeon makes an incision in the patient’s abdomen to access the spine.
To have a clear view of the spine, the surgeon then retracts the abdominal and vascular structures.
Disc Removal
Once the spine is in view, the surgeon removes a portion of the degenerated disc from the affected disc space.
Once the spine is in view, the surgeon removes a portion of the degenerated disc from the affected disc space.


Material Placement
After this disc material is removed, the surgeon inserts bone graft material into the disc space such as autograft or INFUSE® Bone Graft contained in a LT-CAGE® Lumbar Tapered Fusion Device to restore the normal anatomic condition of the spine.
After this disc material is removed, the surgeon inserts bone graft material into the disc space such as autograft or INFUSE® Bone Graft contained in a LT-CAGE® Lumbar Tapered Fusion Device to restore the normal anatomic condition of the spine.
After Surgery
After the surgery, the patient will normally stay in the hospital between 2 to 5 days. The specific time of stay in the hospital will depend on the patient and the surgeon’s specific post-operative treatment plan. The patient will normally be up and walking in the hospital by the end of the first day after the surgery. Your surgeon will have a specific post-operative recovery / exercise plan to help you return to normal life as soon as possible.
Lumbar Microdisectomy
What is it?
Lumbar microdiscectomy is an operation on the lumbar spine performed using a surgical microscope and microsurgical techniques. A microdiscectomy requires only a very small incision and will remove only that portion of your ruptured disc which is “pinching” one or more spinal nerve roots. The recovery time for this particular surgery is usually much less than is required for traditional lumbar surgery.
Why is it done?
Lumbar microdiscectomy is usually recommended only when specific conditions are met. In general, surgery is recommended when a ruptured disc is pinching a spinal nerve root(s) and you have:
- Leg pain which limits your normal daily activities
- Weakness in your leg(s) or feet
- Numbness in your extremities
- Impaired bowel and/or bladder function
The Operation
Incision
In the operating room, a lumbar microdiscectomy begins with a small incision in your lower back. Through this opening, your surgeon will insert microsurgical instruments. Because the work is viewed through a microscope, this approach requires a relatively small incision.
Reaching The “Pinched” Nerve
Guided by diagnostic studies, your surgeon will remove a small portion of bony material from the back of your vertebra. Once this material is removed, the surgeon can locate the exact area where the nerve root is being pinched.
Guided by diagnostic studies, your surgeon will remove a small portion of bony material from the back of your vertebra. Once this material is removed, the surgeon can locate the exact area where the nerve root is being pinched.
Identifying the Cause of the Pressure
Once the “pinched” nerve is located, the extent of the pressure on the nerve can be determined. Using microsurgical procedures, your surgeon will remove the ruptured portion of the disc and any disc fragments which have broken off from the main disc. The amount of work required to complete your microdiscectomy will depend in part on the number of disc fragments present and the difficulty presented in finding and removing them.
Once the “pinched” nerve is located, the extent of the pressure on the nerve can be determined. Using microsurgical procedures, your surgeon will remove the ruptured portion of the disc and any disc fragments which have broken off from the main disc. The amount of work required to complete your microdiscectomy will depend in part on the number of disc fragments present and the difficulty presented in finding and removing them.
Closing the Incision
The operation is completed when each layer of the incision is closed with suture material (stitches) or surgical staples. If the outer incision is closed with staples or non-absorbable sutures, they will have to be removed after the incision has healed
Laminectomy
What is It?
Lumbar laminectomy is an operation performed on the lower spine to relieve pressure on one or more nerve roots. The term is derived from lumbar (lower spine), lamina (part of the spinal canal’s bony roof), and -ectomy (removal).
Why is it Done?
Pressure on a nerve root in the lower spine, often called nerve root compression, causes back and leg pain. In this operation the surgeon reaches the lumbar spine through a small incision in the lower back. After the muscles of the spine are spread, a portion of the lamina is removed to expose the compressed nerve root(s).Pressure is relieved by removal of the source of compression part of the herniated disc, a disc fragment, a tumor, or a rough protrusion of bone, called a bone spur.
What Happens Afterwards?
Successful recovery from lumbar laminectomy requires that you approach the operation and recovery period with confidence based on a thorough understanding of the process. Your surgeon has the training and expertise to correct physical defects by performing the operation; he and the rest of the health care team will support your recovery. Your body is able to heal the involved muscle, nerve, and bone tissues. Full recovery, however, will also depend on your having a strong, positive attitude, setting small goals for improvement, and working steadily to accomplish each goal.
The Operation
Incision
Surgery for lumbar laminectomy is performed with the patient lying on his abdomen or side. A small incision is made in the lower back.
Laminectomy
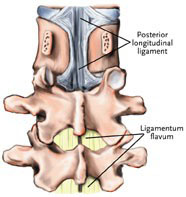
After a retractor is used to pull aside fat and muscle, the lamina is exposed. Part of it is cut away to uncover the ligamentum flavum – a ligament that supports the spinal column.
After a retractor is used to pull aside fat and muscle, the lamina is exposed. Part of it is cut away to uncover the ligamentum flavum – a ligament that supports the spinal column.
Entering the Spinal Canal
Next an opening is cut in the ligamentum flavum through which the spinal canal is reached. The compressed nerve is now seen, as is the cauda equina (bundle of nerve fibers) to which it is attached. The cause of compression may now also be identified – a bulging, ruptured or herniated disc, or perhaps a bone spur.Sometimes a fragment of disc has moved away from the disc space to press on the nerve root as it leaves the spinal canal. This will often cause more severe symptoms. Because of its distance from the disc space, the fragment may not be seen on a myelogram, and a CT scan (CAT scan) may be required to locate it.
Removal of the Herniated Disc
The compressed nerve is gently retracted to one side, and the herniated disc is removed. As much of the disc is taken out as is necessary to take pressure off the nerve. Some surgeons will remove all “safely available” disc material. After the cause of compression is removed, the nerve can begin to heal. The space left after removal of the disc should gradually fill with connective tissue.
Fusion and Instrumentation
Incision Closure
The operation is completed when the incision is closed in several layers. Unless absorbable suture material is used, the skin sutures (stitches) will have to be removed after the incision has healed.

Transforminal Lumbar Interbody Fusion (TLIF)
What is it?
Transforaminal Lumbar Interbody Fusion (TLIF) is an operation where the lumbar spine is approached from the side through an incision in the back. A portion of bone and disc are removed from the spine and replaced with an implant that is inserted into the disc space. Titanium or stainless steel screws and rods are inserted into the spine to ensure the stability of the entire construct.
Why is it done?
Patients who are suffering from back and/or leg pain are potential candidates for the TLIF procedure. The causes of the pain may range from a natural degeneration of the disc space to some type of traumatic event.
The Operation
The operation is performed with the patient laying on his or her stomach.
Incision
An incision is made in the patient’s back to allow the surgeon access to the spine.
The surgeon separates the muscle and tissue to be able to have a clear view of the spine.
Bone is Removed
Once the spine is in view, the surgeon will remove a portion of bone from the appropriate areas of the spine to allow the surgeon to access the disc space.
Disc is Removed
The surgeon will remove the disc material to allow the surgeon to insert an implant into the disc space.
Implants are Inserted
The surgeon will also insert titanium or stainless steel implants into the spine. The implant and the screws will help to restore the spine back to its normal anatomic condition.
After Surgery
After the surgery, the patient will normally stay in the hospital between 3-5 days. The specific time of stay in the hospital will depend on the patient and the surgeon’s specific post-operative surgical plan. The patient will normally be up and walking in the hospital by the end of the first day after the surgery. Your surgeon will have a specific post-operative recovery / exercise plan to help you return to normal life as soon as possible.
Posterior Interbody Lumbar Fusion (PLIF)
As with all spinal fusion surgery, a posterior lumbar interbody fusion (PLIF) surgery involves adding bone graft to an area of the spine to set up a biological response that causes the bone to grow between the two vertebral elements and thereby stop the motion at that segment. Unlike the posterolateral gutter fusion, the PLIF achieves spinal fusion in the low back by inserting a bone graft and/or spinal implant (e.g. cage) directly into the disc space. When the surgical approach for this type of procedure is from the back it is called a posterior lumbar interbody fusion (PLIF). A PLIF fusion is often supplemented by a simultaneous posterolateral spine fusion surgery.
Posterior lumbar interbody fusion surgery description
First, the spine is approached through a three-inch to six-inch long incision in the midline of the back and the left and right lower back muscles (erector spinae) are stripped off the lamina on both sides and at multiple levels. After the spine is approached, the lamina is removed (laminectomy) which allows visualization of the nerve roots. The facet joints, which are directly over the nerve roots, may then be undercut (trimmed) to give the nerve roots more room. The nerve roots are then retracted to one side and the disc space is cleaned of the disc material. A bone graft, or anterior interbody cages with bone, is then inserted into the disc space and the bone grows from vertebral body to vertebral body. Doing a pure PLIF spine surgery has the advantage that it can provide anterior fusion of the disc space without having a second incision as would be necessary with an anterior/posterior spine fusion surgery. However, it has some disadvantages:
- Not as much of the disc space can be removed with a posterior approach (from the back).
- An anterior approach (from the front) provides for a much more comprehensive evacuation of the disc space and this leads to increase surface area available for a fusion.
- A much larger bone graft and/or spinal implant can be inserted from an anterior approach
- In cases of spinal deformity (e.g. isthmic spondylolisthesis) a posterior approach alone is more difficult to reduce the deformity
- There is a small but finite risk that inserting a bone graft or cage posteriorly will allow it to retropulse back into the canal and create neural compression
PLIF surgery rates are higher than posterolateral fusion rates because the bone is inserted into the anterior portion (front) of the spine. Bone in the anterior portion fuses better because there is more surface area than in the posterolateral gutter, and also because the bone is under compression. Bone in compression heals better because bone responds to stress (Wolff’s law), whereas bone under tension (posterolateral fusions) does not see as much stress.